But Biden's statement also makes it easier for his administration to quietly distance itself from mask mandates, whose scientific basis continues to fall under methodological scrutiny.
The so-called Bangladesh mask study,
widely touted in the media as the first randomized controlled trial (RCT) to show small but meaningful protection at least from surgical masks, is the subject of a new
peer-reviewed "re-analysis" in the Springer Nature journal Trials.
Lead author Ben Recht, a University of California Berkeley machine-learning professor, expanded on his
methodological criticisms of the study last year with Carnegie Mellon University mathematician
Wesley Pedgen, who has also scrutinized mask research, and University of Pittsburgh computational biologist Maria Chikina.
"Since high impact publications often lead to changes in social behaviors and government policies, they need to be carefully vetted," they wrote, referring to the
December paper in Science led by Yale economist Jason Abaluck, based on a cluster RCT of 600 Bangladeshi villages.
Social media giants and the federal public health establishment were already protecting mask mandates from scientific challenge when Abaluck's preprint came out in September 2021.
At the same time it was coordinating with the feds to remove purported misinformation,
Twitter locked then-Harvard epidemiologist Martin Kulldorff out of his account for a month for saying elderly people had died because of false claims by public health officials that masks would protect them. Then-National Institutes of Health Director
Francis Collins put Kulldorff on a quasi-blacklist of "fringe epidemiologists" the prior autumn.
"We find that staff behavior in both unblinded and supposedly blinded steps caused large and statistically significant imbalances in population sizes," the Trials paper said of Abaluck's team.
Neither the preprint nor the peer-reviewed paper from the Bangladesh study included the "raw numbers" from the trial, though Abaluck posted them after initial media coverage, showing "the primary outcome [symptomatic seropositives] differed by a total of just 20 cases between the treatment and control arms" in a study population of 300,000, Recht and the others wrote.
"In particular, the difference in rates is constituted by denominator differences, and thus is similar in magnitude (10% vs 9%) to the population imbalance which arose through the interaction of staff bias and random chance (156,938 and 170,497 individuals enrolled in control and treatment respectively)," the paper says.
It notes that Abaluck's team already conceded the study had "substantial post-randomization ascertainment bias" due to staff who were "tasked with both enrolling households and providing masks in the treatment villages and hence were aware whether they were surveying a treatment or control village." But this bias could only "account for 25% of the difference in size between treatment and control," suggesting "some unintentional unblinding" as well.
"The purpose of randomized control trials is to establish a causal link between interventions and outcomes," notes the Trials paper. "However, causal implications are diminished in the presence of unblinding, ascertainment bias, and bias-susceptible endpoints. Unfortunately, in the Bangladesh mask trial we [find] evidence of all of the above."
University of California San Francisco epidemiologist Vinay Prasad, who previously wrote his own review of mask-research literature,
called the reanalysis "provocative" in his newsletter. The Bangladesh study "falls apart," he concluded.
"If participants could see a big truck or boxes in intervention villages, but not see that in control villages, they may be more likely to enroll," he wrote. "In fact, 9% more likely!"
A person who enrolls in the trial because "they are getting something for free" may be "slightly less likely to properly report COVID symptoms (perhaps they report less or differently) and less likely to follow through with testing," Prasad said. "Assuming these people are just a little different, can cause the entire trial results to tip."



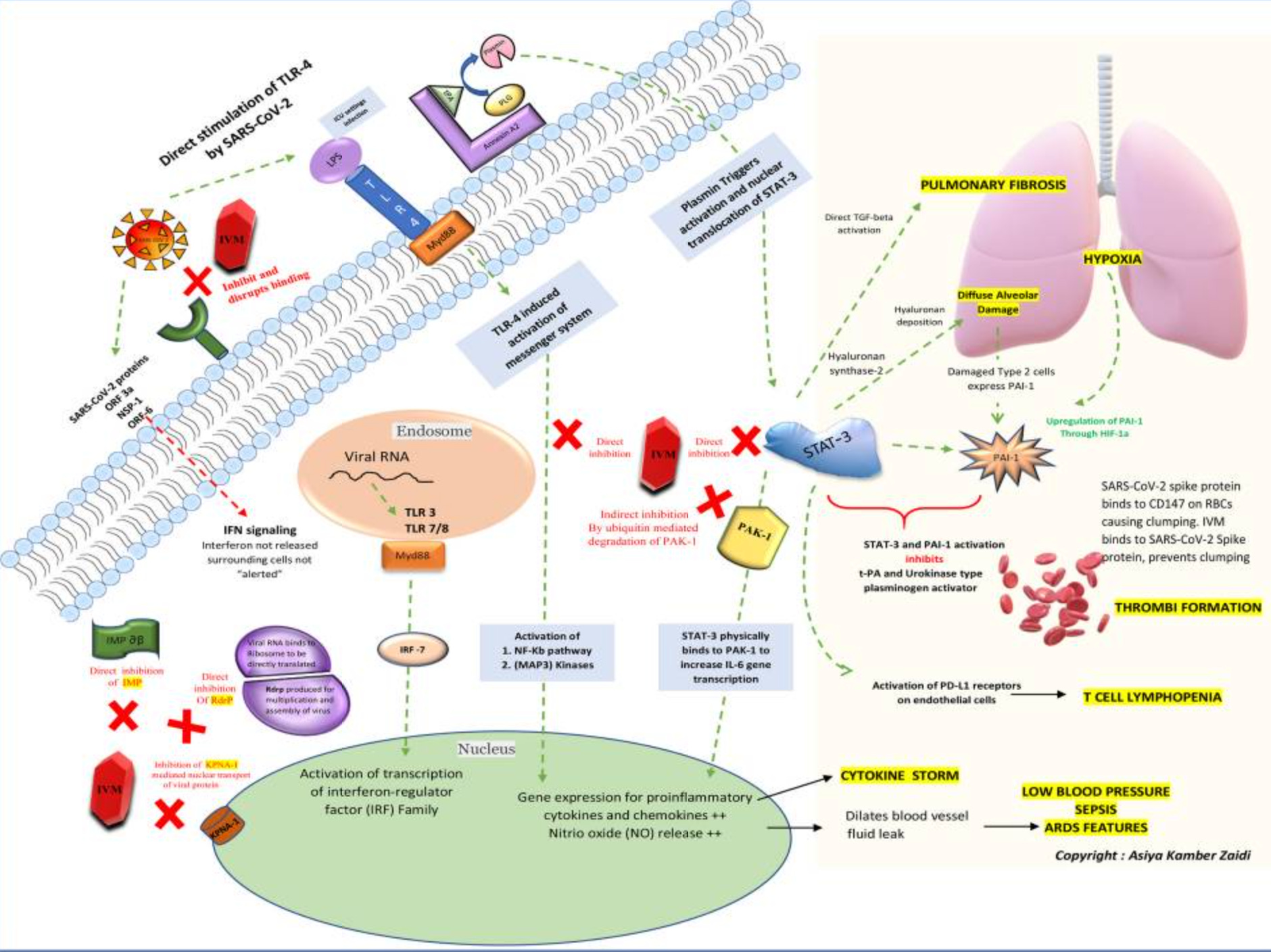
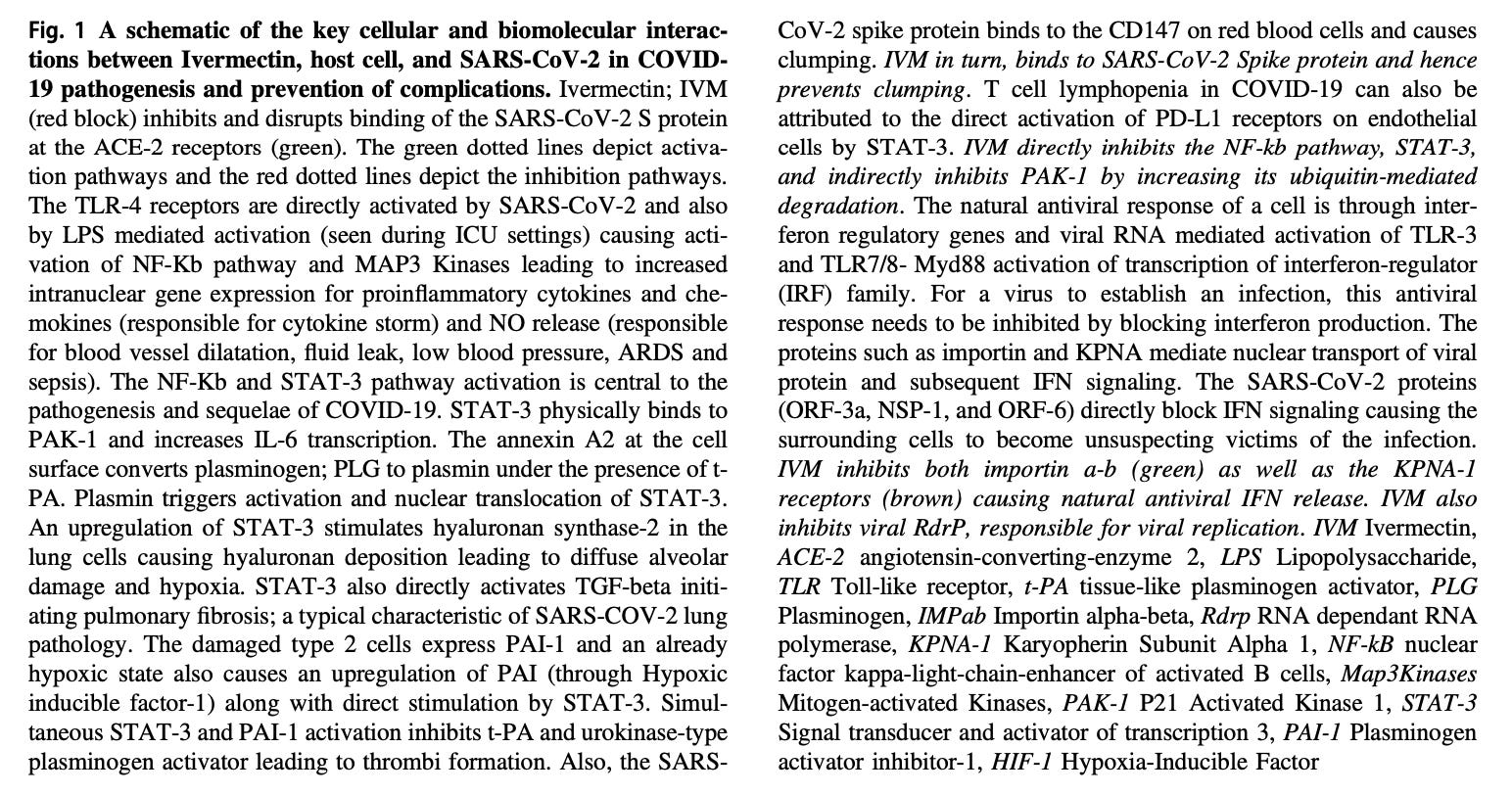
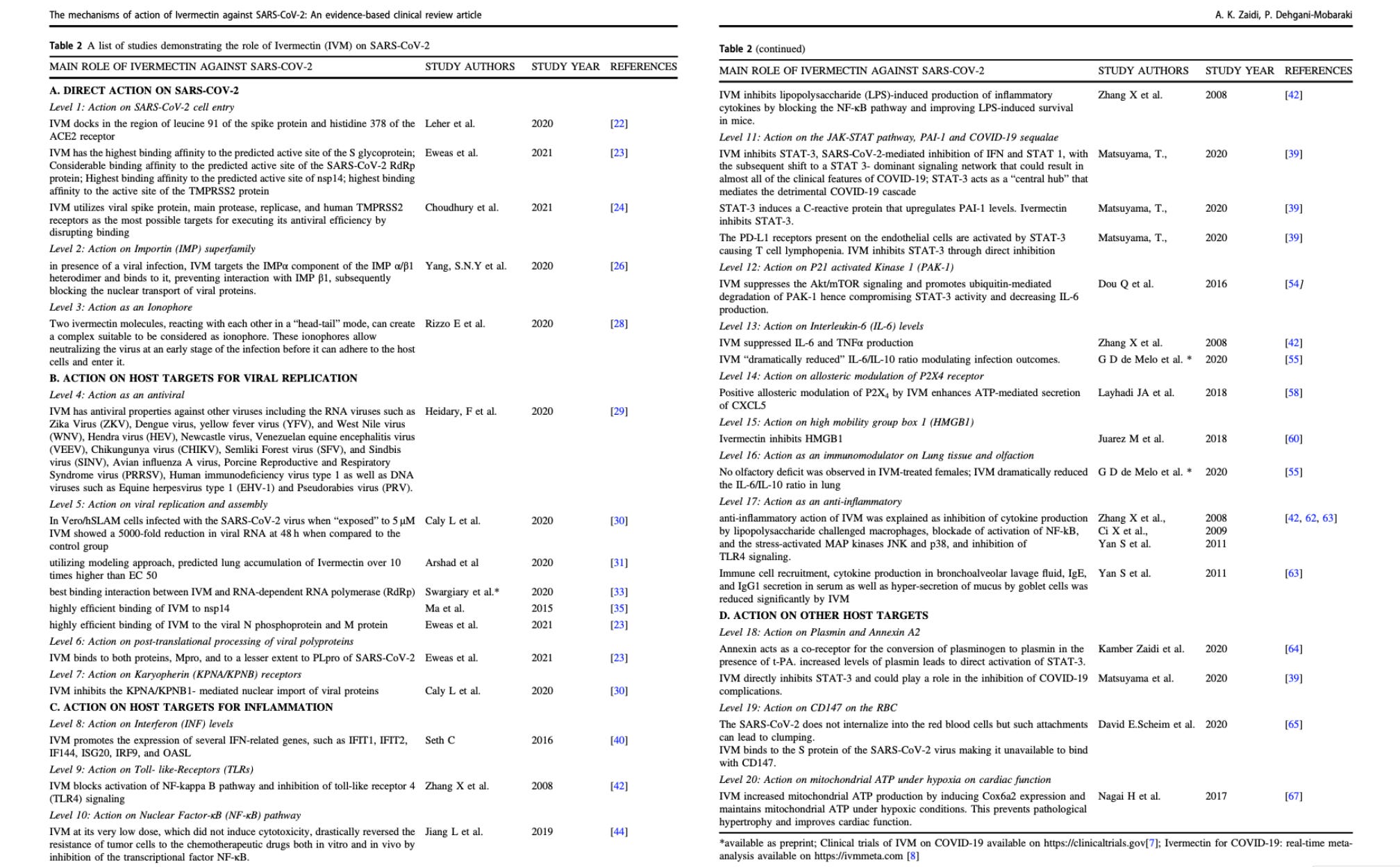
 You may have seen articles this weekend about a new peer-reviewed study of over 80,000 patients taking Ivermectin in Brazil, published in Cureus, titled “Regular Use of Ivermectin as Prophylaxis for COVID-19 Led Up to a 92% Reduction in COVID-19 Mortality Rate in a Dose-Response Manner: Results of a Prospective Observational Study of a Strictly Controlled Population of 88,012 Subjects.”
You may have seen articles this weekend about a new peer-reviewed study of over 80,000 patients taking Ivermectin in Brazil, published in Cureus, titled “Regular Use of Ivermectin as Prophylaxis for COVID-19 Led Up to a 92% Reduction in COVID-19 Mortality Rate in a Dose-Response Manner: Results of a Prospective Observational Study of a Strictly Controlled Population of 88,012 Subjects.”